The Fear Behind the Food: Untangling ARFID and Emetophobia Diagnoses


The fear of vomiting can drive powerful food avoidance and the diagnostic picture is not always straightforward. In some cases, we are looking at Avoidant/Restrictive Food Intake Disorder (ARFID). In others, it may be emetophobia, a Specific Phobia centered around vomiting. To add to that complexity, while not a focus of this blog post, Obsessive-Compulsive Disorder (OCD), often contamination-focused, may also be part of the clinical picture. These diagnoses can present independently; however, frequently co-occur and the overlap in symptoms can become very confusing. We know that accurate conceptualization shapes access to effective treatment, which makes careful assessment and differentiation important.
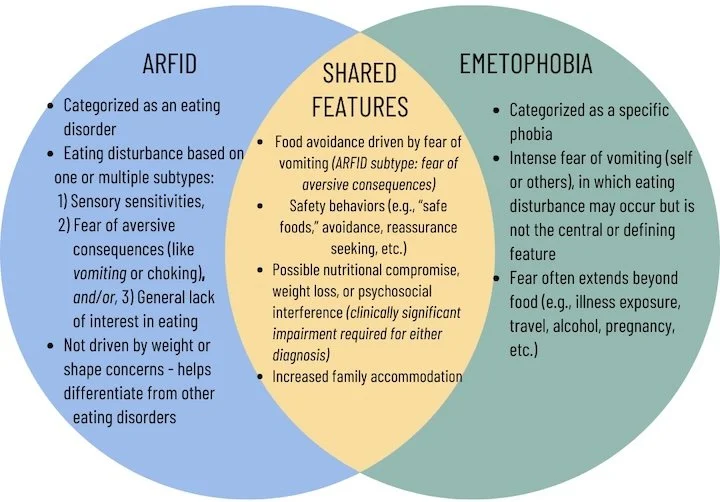
ARFID is an eating disorder characterized by a disturbance in eating that is not driven by concerns about weight or body shape. Instead, food avoidance may stem from sensory sensitivities, low appetite or lack of interest in food, or fear of aversive consequences (e.g., vomiting, choking, or allergic reactions). When fear of vomiting is present in the case of fear of aversive consequences, individuals may avoid foods they associate with nausea, contamination, or past illness to name a few. For some, this fear emerges after a particularly distressing or traumatic experience related to eating, strengthening the belief that certain foods are unsafe. In ARFID, the core clinical issue is the disturbance in eating itself.
In cases of emetophobia, this is considered a specific phobia of vomiting (self or others). While food may become restricted, that is not always the case, and the fear often extends beyond eating. Individuals may avoid anyone who appears ill, travel, pregnancy, alcohol, or other triggering cues or environments. There is typically heightened vigilance to bodily sensations such as nausea or stomach discomfort, with these sensations interpreted as signs that vomiting is imminent. In emetophobia, the primary driver is the fear of the vomiting event itself, rather than a broader disturbance in eating.
The diagram I created below illustrates the clinical overlap between these two diagnoses. Both can involve significant food avoidance and, in some cases, weight loss or nutritional concerns. However, the key distinction lies in the role that eating disturbance plays in the overall presentation. In ARFID, the diagnosis requires either nutritional compromise, significant weight loss, dependence on supplements, or psychosocial interference. Whereas with emetophobia, eating may be affected and weight loss can occur, but these are not as central to the diagnosis. Although, there still must be clinically significant distress or impairment in functioning.
In both ARFID (fear of aversive consequences subtype) and emetophobia, anxiety decreases in the short term when the feared foods or situations are avoided, but that temporary relief reinforces the cycle and strengthens fear over time. The same avoidance pattern maintains both conditions, which is why exposure is a key ingredient in effective treatment. For ARFID, this could look like structured work to face feared foods or textures, increase food variety, and restore adequate nutrition, which are core elements of Cognitive Behavioral Therapy for ARFID (CBT-AR). For emetophobia, Exposure with Response Prevention (ERP) is considered the gold standard treatment, helping individuals gradually face feared sensations and situations while reducing safety behaviors. Importantly, when food restriction is present, careful attention to medical and nutritional status is critical. Regardless of diagnosis, inadequate intake or weight loss can have meaningful physical consequences and should be assessed and monitored as part of comprehensive care, including coordination with medical providers.
Interested in further assessment or consultation on this topic? Get connected with Dr. Rogers below.
References
American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Fifth ed. 2013, Arlington, VA: American Psychiatric Publishing.
Thomas, J.J. & Eddy, K.T. (2019). Cognitive-Behavioral Therapy for Avoidant/Restrictive Food Intake Disorder: Children, Adolescents, & Adults. Cambridge: Cambridge University Press.
Zickgraf, H.F., Murray, H.B., & Rigby, A. (2025). Avoidant/restrictive food intake disorder symptoms are common and impairing in adults with specific phobia of vomiting: An exploratory study in an understudied population. Psychological Reports. Advance online publication.