The Role of Exposure in Trauma Treatment


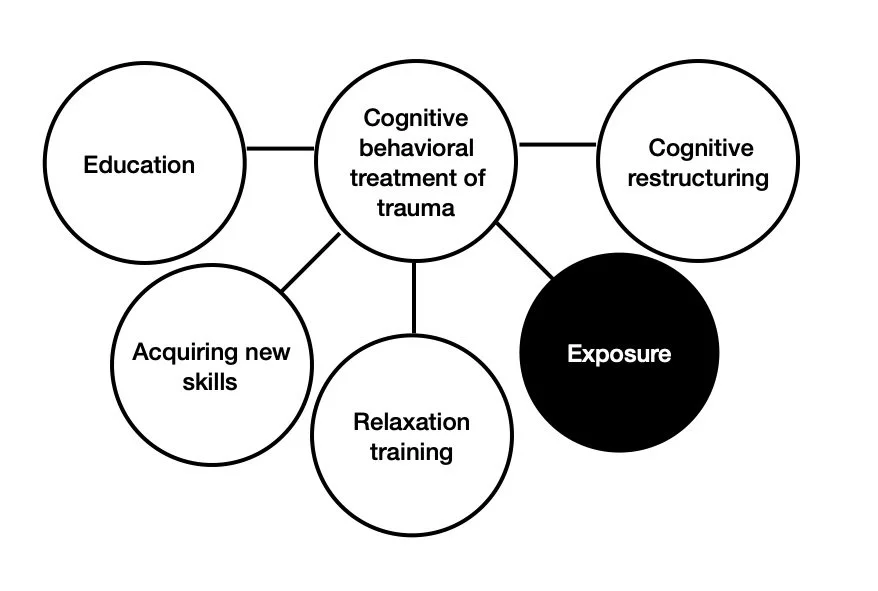
Cognitive behavioral treatment of trauma usually consists of multiple interventions that help individuals feel safe in the current moment, make sense of what happened to them, understand the impact of trauma on the brain, think in more helpful ways, and reduce avoidance. This blog post will focus on exposure as a core component of treatment for trauma-related symptoms, so that you can better understand this important aspect of CBT for trauma.
First, it is important to remember that about 94% of people that experience at traumatic event do not have post-traumatic symptoms (Koenen et al., 2017). So, what is different between those people that experience a traumatic situation and have post-traumatic symptoms, and those that experience something traumatic and do not? Post-traumatic symptoms (e.g., flashbacks, intrusive memories, fear at reminders of the trauma) are common after a traumatic experience. However, those who recover without treatment are repeatedly exposed to trauma memories and reminders, allowing for their brain to emotionally process the event (Foa & Cahill, 2001). Natural exposures to trauma reminders in the form of thinking about what happened and talking with friend and family allows the brain to learn the difference between the trauma (in the past) and the reminders of the trauma (in the present).
Those who go on to have chronic PTSD symptoms may see non-threatening reminders of the trauma as dangerous, leading to avoidance of these reminders (Foa et al., 2007). When an individual avoids both external reminders (locations, people, objects, activities) and internal reminders (memories, emotions, thoughts) of the trauma, they do not allow for their brain to learn that these reminders are not dangerous. In other words, the brain does not get new information to learn that reminders of the trauma are not the trauma.
So, if avoidance is one factor that maintains PTSD symptoms, what is the intervention that may work best? Exposure to internal and external reminders of the trauma is often a key component of trauma treatment, as it blocks the avoidance that is maintaining trauma symptoms. Safely approaching reminders of the trauma allows for 1) your brain to learn the difference between the trauma and reminders of the trauma, 2) allows you to learn that your anxiety will go down over time, 3) allows you to examine unhelpful beliefs about the traumatic event, and 4) allows you to reclaim your life again after a traumatic event (Foa et al., 2007).
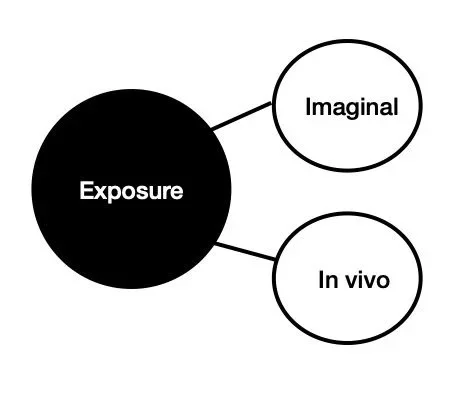
There are two types of exposure that are important in trauma treatment: imaginal (in imagination) and in vivo (in real life) (Foa et al., 2019; Tuvia & Rego, 2017). Imaginal exposure looks like recounting trauma memories in session with your therapist and discussing the emotions and beliefs that are raised when recounting the memory. This allows you to approach trauma memories in a safe way to disconfirm beliefs that remembering the trauma is dangerous. In vivo exposure means confronting real-life, safe situations that remind you of the traumatic event. In treatment, you and your therapist will agree on an “exposure hierarchy”, which is a list of feared situations, activities, or objects that you will confront outside of session for homework. This list will start with things that you are less afraid of, and, over time, you will work your way through the hierarchy. If you want to learn more about exposure treatment for trauma, the APA website has a great overview here: https://www.apa.org/ptsd-guideline/treatments/prolonged-exposure.
In my work with clients, I assess what is keeping them stuck and use a evidence-based cognitive behavioral interventions to alleviate symptoms. This may include exposure, but also likely includes helping you change the way you think (cognitive restructuring), helping you learn new skills, and education about how the brain and mind work. If you are interested in learning more about how trauma treatment looks for my clients, you can read this blog post: https://www.findyourbase.com/blog/11/2025/dr-judith-hermans-three-stages-of-trauma-treatment-in-practice.
If you are interested in evidence-based trauma treatment, don’t hesitate to schedule an intake with Dr. Alexandra Halberstadt!
References
Foa, E. B., & Cahill, S. P. (2001). Psychological therapies: Emotional processing. In N. J. Smelser & P. B. Bates (Eds.), International encyclopedia of the social and behavioral sciences (pp. 12363-12369). Oxford: Elsevier.
Foa, E.B., Hembree, E.A., & Rothbaum, B.O. (2007). Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences. Oxford University Press.
Foa, E. B., Hembree, E. A., Rothbaum, B. O., & Rauch, S. A. M. (2019) Prolonged Exposure Therapy for PTSD: Emotional processing of Traumatic Experiences - Therapist Guide (2nd Edition). Oxford.
Koenen, K. C., Ratanatharathorn, A., Ng, L., McLaughlin, K. A., Bromet, E. J., Stein, D. J., Karam, E. G., Meron Ruscio, A., Benjet, C., Scott, K., Atwoli, L., Petukhova, M., Lim, C. C. W., Aguilar-Gaxiola, S., Al-Hamzawi, A., Alonso, J., Bunting, B., Ciutan, M., de Girolamo, G., Degenhardt, L., … Kessler, R. C. (2017). Posttraumatic stress disorder in the World Mental Health Surveys. Psychological medicine, 47(13), 2260–2274. https://doi.org/10.1017/S0033291717000708
Tuvia, T., & Rego, S. (2017). Five Sessions of in Vivo Exposure Therapy for Post-traumatic Stress Disorder: A Case Report. European Psychiatry, 41(S1), S727–S727. doi:10.1016/j.eurpsy.2017.01.1325